
The judge has granted us a hearing on the Motion to Dismiss for Lack of Jurisdiction and the substantive issue of the DMCA take-down notices! It’s due to take place in late June.
The judge has granted us a hearing on the Motion to Dismiss for Lack of Jurisdiction and the substantive issue of the DMCA take-down notices! It’s due to take place in late June.

I often write about the fact that homebirth advocates, despite their claims of being “educated” about childbirth, are generally quite ignorant. They lack the basic knowledge of science, statistics and obstetrics that would allow them to evaluate what they read on the Web (or more importantly, to recognize that you cannot become educated by reading on the Web).
Ignorance is not the only deficiency. Homebirth advocates seem to suffer from a serious problem with magical thinking.
What is magical thinking? It’s the belief that your own thoughts have power to “magically” control events. It’s difficult to imagine anything more emblematic of magical thinking than the inane mantra, “trust birth.”
Does trusting hearts prevent heart attacks? Does trusting pancreases prevent type I diabetes? Does trusting breast prevent breast cancer? Obviously not, so how can any grown woman counsel another with a straight face to “trust birth” as a method of preventing life threatening pregnancy complications? And how can any grown woman actually believe that “trusting birth” is going to have any impact on anything?
The idea that women could actually believe that “trusting birth” will have any impact is especially remarkable considering that most women already recognize that trust has absolutely no impact on miscarriage, the most common life threatening (to the embryo) complication of pregnancy. Indeed, miscarriage demonstrates that the philosophy of “trusting birth” is completely farcical.
Your body is perfectly designed to give birth?
Really? Then why do 1 out of every 5 confirmed pregnancies end in miscarriage?
Miscarriages are commonly caused by devastating genetic defects, such as the absence of a chromosome or an extra chromosome. A some point in the reproductive process, during the formation of the the ovum (or the sperm) or during fertilization, a massive genetic error occurs and that error is incompatible with life. No amount of “trust” can prevent these genetic errors and no amount of “trust” can prevent the miscarriages that result.
Let’s think about what that really means: the same body that is supposedly perfectly designed to give birth will create embryos with the wrong number of chromosomes approximately 20% of the time.
How trusting would you be of an airline if 20% of their flights crashed on takeoff and burned killing all aboard? How trusting would you be of an automobile manufacturer if 20% of their cars blew up the first time you turned the key in the ignition? How trusting would you be of a soup maker if 20% of people who consumed it got botulism and died? I suspect that you wouldn’t be very trusting at all. So how on earth can any woman trust any aspect of pregnancy when it ends in the death of the embryo fully 20% of the time?
How does trusting birth prevent a placenta that can’t transfer oxygen fast enough to a baby during labor? How does trusting birth prevent a breech baby’s head from getting stuck, killing the baby? How does trusting birth prevent the mother from having a stroke because of pre-eclampsia, killing her? Obviously it can’t prevent any of those things because “trusting birth” is nothing more than immature wishful thinking.
Why on earth would you think that a process that can’t even manage to assemble the correct number of chromosomes more than 20% of the time is going to result in a baby who fits perfectly, has a perfect placenta, and develops no life-threatening complications?
Simply put, how could any grown woman, with a modicum of intelligence “trust birth”? And how could any grown woman, with a modicum of intelligence, trust any provider who counseled her to “trust birth”?
Please, enlighten me as to why “trusting birth” isn’t among the stupidest possible prescriptions for a healthy baby and a healthy mother.

Ahh, stuntbirth, also known among aficionados as freebirth or unassisted childbirth (UC).
Stuntbirthers like to pretend to themselves and others that this is how birth happens in nature (no, across all times, places and culture, birth is assisted), that birth is so deeply personal and “sexual” that a couple must experience it alone (really, then why do stuntbirthers post videos of it on YouTube for all the world to see?) and that it is safe. The entire practice would be nothing more than a punch line were it not for the fact that it kills babies. Indeed, both the leading American and Australian advocates of UC, Laura Shanley and Janet Fraser, have ended up with dead babies as a result.
Unassisted childbirth has no benefit for the baby and poses very serious risks. It is a form of medical neglect based on appalling ignorance and extraordinary selfishness and self-absorption. Don’t believe me? Consider Raeanne’s stuntbirth plan, found (where else?) on Mothering. com. Unfortunately, I cannot share the whole inane document, and it will almost certainly be deleted by the folks at MDC when they find that it is being ridiculed, but I can share the high points, starting with the fact that Raeanne dodged a bullet with her first baby (my first was 19 days “late”) and cannot tell the difference between luck and wisdom.
Early labor:
- Make sure everything is cleaned up and in order in the house (no clothes or toys laying around where Raeanne could trip or bleed on them)…
- If laundry needs to be washed throw a load or two in.
- Start dishwasher if needed.
Pretty clever getting her husband to clean the house using labor as an excuse.
Active labor:
- Maybe recommend a shower too? Help her blow dry her hair if she wants…
- Remember that sometimes a red/purple line will appear between a woman’s butt cheeks that can indicate how dilated she is. Check for that! If it is slightly below the tailbone she’s at 6 or 7 cm. if it’s at the top of butt crack she is probably around 10 cm! Take a picture so Raeanne can help you analyse…
- For emergency childbirth procedures refer to Emergency Childbirth by Gregory White!
Yup! In an emergency, just refer to the book. That’ll work.
The baby:
- Make sure baby is breathing!
- The most important thing is skin to skin contact (with a blanket draped over mother and baby), hearing familiar voices, a relaxed atmosphere, leaving the cord attached …
It’s hard to imagine that anyone is so ignorant that they actual believe that the “most important thing” is skin to skin contact, but stuntbirth aficionados are nothing if not gullible.
How about postpartum bleeding?
- If placenta has not been delivered give Angelica: 1 dropper full under the tongue every minute as needed and up to 3 times.
- If placenta has been delivered give Shepherd’s Purse 1 dropper full under the tongue every minute as needed (up to 3 doses) and a dime-sized slice of the maternal side (membrane side that was attached to the uterus) of the placenta to tuck into her cheek and get baby to nurse asap!
- Ice cubes on the bottoms of her feet. This causes strong contraction through the sympathetic nervous system, and it also slows circulation and decreases bleeding.
Really? Really??!!
Hopefully Raeanne and her baby will survive her own stupidity, but, if so, that will only be luck … which Raeanne will never realize because she is an ignorant fool.

Congratulations to the blogger at Hiking the Paper Trail to Parenthood. You win the prize for packing the highest volume of stupid claims into any post of its size!
The blogger, an expectant mother, is so ignorant about childbirth that she is happily transmitting mistruths, half truths and outright lies in her post 8 Things Not To Say to a Crunchy Expectant Mother : A Tirade.
Consider these whoppers:
1. “Women die in hospitals in the US during and after birth.”
Duh. That’s because childbirth is dangerous.
The issue is not whether women die in the hospital during and after childbirth, the issue is the RATE of death compared to the rate of death at homebirth.
2. A completely fabricated, bald faced lie: “The United States of America currently (as of Summer of 2012) has the highest mother and infant mortality rate of every developed country in the world.”
No, not even close. Not to mention that infant mortality is the wrong statistic and that international comparisons of mortality rates are invalid since many countries cheat by counting LIVE premature babies as stillbirths.
3. “Holland, the has some of the best infant and maternal mortality rates in the developed world, with a common 80% of births taking place at home.”
I guess if you are going to make stuff up, you might as well go all the way. The Netherlands has one of the worst perinatal mortality rates in Western Europe and a homebirth rate of 27% and falling. Dutch midwives caring for low risk women (home or hospital) have death rates HIGHER than Dutch obstetricians caring for high risk patients.
4. “My midwives’ rate of patients who end up in Cesarean is less than 4%.”
And what are the death rates of homebirth midwives? Let me guess: the blogger has no clue that LICENSED homebirth midwives attending PLANNED homebirths have death rates up to 800% higher than term hospital birth. Let me guess; the blogger has no clue that the Midwives Alliance of North America (MANA), the organization that represents homebirth midwives refuses to release the death rates of their members because those rates are so hideous.
5. “I have never heard of someone getting a “super germ” like mrsa (a potentially lethal and antibiotic-resistant infection) in their own home.”
Most cases of MRSA (methicillin resistant staph aureus) are “community acquired” not hospital acquired.
6. “Both midwives have the same neonatal resuscitation experience as L&D and NICU staff in a hospital.”
Possibly the stupidest of the many stupid claims in this piece. Most homebirth midwives have NO training in advanced resuscitation, have NO experience in advanced resuscitation, and have NEVER intubated a baby.
7. “There will be medications, IVs and oxygen available if they are needed.”
Will there be an operating room? If not, and you experience a life threatening emergency, your baby will die. Will there be someone skilled in intubation and advanced neonatal resuscitation? If not, and your baby is born needing more than a little oxygen, your baby may die or suffer permanent brain injury. Will there be blood for transfusions? If not, you can hemorrhage to death long before you get to the nearest hospital.
8. “The people who ask this question are the ones to whom information and education have no impact.”
No, honey, you are the one on whom information and education have had no impact because you are the one who hasn’t been exposed to either information or education. Reading the lies of other homebirth advocates on the internet and gullibly believing them is not “education,” it is merely a sign of lack of basic knowledge of science, statistics and childbirth.
Here’s some real information you can use:
Planned homebirth with an American homebirth midwife is the MOST dangerous form of planned birth in the US.
Take down your post, which is utter crap, stop spewing arrant nonsense, and learn some actual facts about childbirth. I guarantee you will be very, very surprised.

Breastfeeding is a good thing. I heartily endorse it; I did it with four children; I really enjoyed it.
But it isn’t nearly as good as lactivists have implied. For example, all those long term health benefits of breastfeeding that you’ve heard about? None of them exist.
Don’t believe me? Perhaps you will believe the World Health Organization.
The World Health Organization recently published Long-term effects of breastfeeding; a systematic review by Horta and Victora. It is a 74 page paper, but it can be summed up in one sentence:
There is no evidence for any long term health benefits of breastfeeding.
The paper is an evaluation of the entire world literature on the long term benefits of breastfeeding and it is divided into individual sections for each purported benefit. These include overweight and obesity, blood pressure, serum cholesterol, type-2 diabetes, and intellectual performance.
In every case, the scientific literature does not support a claim of benefit.
Specifically:
1. Overweight and obesity
Our conclusion is that the meta-analysis of higher-quality studies suggests a small reduction, of about 10%, in the prevalence of overweight or obesity in children exposed to longer durations of breast-feeding. Nevertheless, it is not possible to completely rule out residual confounding because in most study settings breastfeeding duration was higher in families where the parents were more educated and had higher income levels.
In other words, the observed effect is very small and probably due entirely to confounding.
2. Blood pressure
[The] findings are consistent with a small protective effect of breastfeeding against systolic bloodpressure, but residual confounding cannot be ruled out.
Once again, the observed effect is small and probably due entirely to confounding.
3. Cholesterol
Because the confidence interval included the null effect, these results do not support a long-term programming effect of breastfeeding on blood lipids.
4. Type-2 diabetes
The evidence suggests that breastfeeding may have a protective effect against type-2 diabetes,particularly among adolescents. Obesity/overweight seems to account for part of the association. Generalization from these findings is restricted by the small number of studies and the presence of significant heterogeneity among them.
5. IQ
[A]mong those studies that adjusted for maternal intelligence, breastfeeding was associated with an additional 2.19 IQ points… [T]he practical implications of a small increase in the performance in intelligence tests may be open to debate.
Since IQ tests are generally acknowledged to have a standard error of 3 points, there is no difference.
*****
These results are not news. The new study merely confirms the results from the original WHO study of the same name published in 2007.
These results are not surprising. With the exception of IQ testing, the studied outcomes are risk factors for diseases of adulthood and old age.Throughout most of human existence, life span was approximately 35 years, and diseases of old age had little to no impact on the survival of the species. There is no reason to expect there would be much of an evolutionary advantage to avoiding the disease of old age.
In industrialized societies, the benefits of breastfeeding are small and short term. That’s why there is no reason for any mother who chooses bottlefeeding to feel guilty. Breast milk is not “liquid gold.” It’s just milk and confers a few small, short term benefits across populations compared to infant formula.

Yoni cupcakes.
Yes. It’s just what it sounds like. Perfect for the Blessingway preceding your all natural breech homebirth of twins after 6 C-sections.
The picture is not suitable for work. You can click here to see it.
Beware. Once seen, it cannot be unseen.

On Monday Techdirt published yet another piece on my lawsuit against Gina, MPAA Freaks Out: Insists That Having To Consider Fair Use Before Filing A DMCA Takedown Would Be Crazy:
Is it really any surprise that the MPAA suddenly took notice of the case after the EFF filed an amicus brief? The MPAA had to step in and argue why it should be allowed to continued to file millions of DMCA takedowns without having to be that careful about bogus takedowns, because actually having to make sure a work is infringing would be too much work. So, the MPAA basically says, “we should be allowed to stifle free speech with no consequence because OMG PIRACY@!@!!” Yes, that’s a paraphrase, but that’s the crux of the MPAA’s argument.
Like most everything else Techdirt has written about the lawsuit, it gets to the heart of the matter. However, like other published reports on the lawsuit, it gives short shrift to the underlying dispute, claiming that it is silly. I’d like to explain why the underlying dispute is not silly at all, but is deadly serious.
I imagine that people unfamiliar with the history of the case might have been thrown off by the fact that it was triggered by Gina’s incredibly immature posting of herself making an obscene gesture to me, but that was simply the way that she learned about the DMCA process; it has nothing to do with the underlying issue.
As I detail in the legal briefs, the underlying issue is that Gina wanted to silence my voice on the Web because she disagrees with what I have to say. She’s not alone in her feelings; I am anathema in natural childbirth circles because I aggressively challenge their attempts to deny the historical and scientific evidence that shows childbirth is and has always been inherently dangerous, modern obstetrics has dramatically reduced both maternal and neonatal mortality, and most of what NCB advocates believe is stuff that they simply made up.
In my efforts I am no different from paleontologists fighting against advocates of intelligent design; no different from climate scientists fighting against those who would deny global warming; and no different than physicians fighting against anti-choice activists claim (erroneously) that abortions cause everything from breast cancer to depression.
Perhaps at first blush the lawsuit appears to be about two women arguing over “women’s stuff.” But this “stuff” is a matter of life and death. On a regular basis I share stories of babies and mothers who have died because women rejected medical science at the behest of natural childbirth advocates. Far from being silly, the underlying dispute is deadly serious.
If someone can abuse the DMCA process to silence me, it opens the way to others using the DMCA process to silence the immunologists, pediatricians and public health professionals who promote vaccination. It opens the way for climate denialists to use the DMCA process to silence the professionals who have warned us about global warming. And it opens the way for anti-choices activists to use the DMCA process to silence the doctors who point out their lies.
This is about something far more serious than the immature gesture of one blogger now immortalized in the Federal Court Files. It’s about protecting those who convey scientific evidence from those who prefer to pretend that scientific evidence doesn’t exist.

It seems like every natural childbirth blog or book has a list of “Steps to a Joyful Birth.” I find this surprising since I never considered that there was anything necessary for a joyful birth besides a desired baby.
But since everyone else is doing it, and since I’ve witnessed thousands of joyful births, as well as had four exceedingly joyous births of my own children, I thought I’d offer my set of steps.
1. Don’t read the NCB literature
One of the most striking things about women who are disappointed in the birth of a healthy, wanted baby is their disappointment is usually connected to the fact that their birth did not meet the arbitrary “standards” set by natural childbirth advocates.
I’ve read a lot of the natural childbirth literature and I can tell you that most of it is guilt-inducing lies. In the first place, NCB has no basis in either science or reality; its fundamental claims are nothing more than stuff that advocates made up to valorize their own personal choices. Moreover, NCB was fabricated by Grantly Dick-Read, a white, male eugenicist whose goal was to trick women of the “better” classes into having more children by telling them that the pain of labor was all in their heads.
Reading the NCB literature to find out what your birth ought to be like is the equivalent of reading Vogue Magazine to determine what your body ought to look like. It’s almost guaranteed to end in disappointment.
2. Don’t make a birth plan
Birth plans are worse than useless. They’re useless because they are as effective as making a “weather plan” and for the exact same reason. You have no control over how your labor will progress (or not progress) and you certainly have no control over how well your baby will tolerate that labor.
As I’ve noted in the past, birth plans engender hostility from the staff, are usually filled with outdated and irrelevant preferences, and create unrealistic expectations among expectant mothers. But the worst thing about birth plans is they don’t work. They don’t accomplish their purported purpose, make no difference in birth outcomes, and, ironically, predispose women to be less happy with the birth than women who didn’t have birth plans.
3. Don’t make any plans about pain medication until you feel the pain
Sounds obvious, right? You wouldn’t make demands about how much pain medication you will or will not take after your root canal; you’d wait until you experienced the pain and then tailor the amount of pain medication, if any, to whether you felt you needed it. Why on earth would you decide to refuse pain medication for labor until you’ve felt the pain? I know why; because once you feel the pain you’ll want the medication and the only way that NCB advocates can get you to mirror their choices is to convince you to refuse pain medication before you have any idea what the pain will be like.
Making an important decision like this, before you have accurate information is a set up for disappointment.
4. Don’t hire anyone, midwife, doula or childbirth educator, who values process over outcome
They will try to convince you that there is one BEST way to give birth and that you should feel disappointed if you don’t meet their arbitrary goal. Who needs that?
5. Don’t expect to be immediately smitten by overwhelming love for your baby
Let’s see. You’ve just spent the past 40 hours suffering an agony that you never even dreamt was possible. You haven’t slept. You haven’t eaten. You’ve thrown up repeatedly. Your nether regions (or your abdomen) feel like they are on fire. You are so tired you can barely lift your head off the pillow. And now you’re supposed to feel overwhelming love for someone you’ve never met before? It might happen, but don’t count on it.
It doesn’t matter whether you feel overwhelming love for your baby immediately after birth. That’s just another one of those NCB fantasies. You might feel that way, or it might take days or weeks to develop. That’s okay. It doesn’t need to happen immediately for you to form an ironclad bond with your baby.
6. Don’t take a good outcome for granted
This is by far and away the most important step. Any baby, especially a healthy baby, is a miracle. When you are counseled to assume that there will be no complications, and your baby will be healthy (“trust birth”) your joy, wonder and gratitude are inevitably diminished.
Homebirth advocates are hypocrites. They tout two diametrically opposed views of risk in an effort to justify their personal preferences.
Homebirth advocates are invariably lactivists. Lactivism is based on the belief, central to attachment parenting, that mothering is about doing whatever it takes to reduce risks to babies to the lowest possible level and doing whatever it takes to promote brain development (real or imagined). Homebirth is about ignoring risks to babies, either by pretending those risks do not exist, or by insisting that there is more to birth than whether a baby is healthy.
Consider:
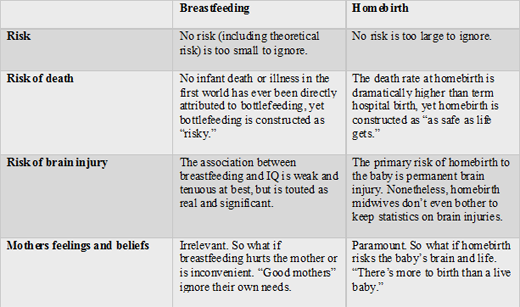
There is not a single infant death in the first world that has ever been attributed to infant formula properly prepared (by both factory and parent), yet homebirth advocates insist that formula is “risky,” should be locked up in hospitals, and, if lactivists had their way, should be available by prescription only. There are dozens of preventable homebirth deaths each year, yet homebirth is constructed as “safe as houses” or “as safe as life gets.”
We live in a society obsessed with “intelligence.” According to homebirth advocates, mothers should breastfeed in order to obtain every last IQ point possible. What about the risk of brain damage at homebirth? It’s never even mentioned. Homebirth midwives don’t bother to keep any statistics on brain injuries that occur at homebirth.
Indeed the entire approach to risk is inverted 180 degrees when comparing breastfeeding and homebirth. In regard to breastfeeding there is literally no “risk” of bottlefeeding too small to be taken into account. Yet when it comes to homebirth, there appears to be no risk too large to be ignored. Breech? VBAC? Twins? Triplets? More risk leads to more kudos.
When it comes to breastfeeding, homebirth advocates consider mothers’ feelings to be irrelevant. There is simply no amount of maternal pain, difficulty or inconvenience that can justify bottle feeding in their minds. Yet the same people see no problem with a mother risking her baby’s death at homebirth because she’s afraid of the hospital, or doesn’t want the discomfort of a heplock.
If it could be shown that a baby died specifically because of bottlefeeding, homebirth advocates would be up in arms. When a baby dies at homebirth, advocates tell each other that the baby was “meant” to die. Formula manufacturers are evil; homebirth midwives who preside over preventable perinatal deaths, even multiple perinatal deaths, are “persecuted.”
There is one area that homebirth advocacy and lactivism share in common, though. Both are the personal preferences of privileged white women who have elevated their preferences to an ideal that should be emulated by everyone else.
That’s not surprising. Homebirth and lactivism aren’t about babies; they’re both about mothers and their own self image. Babies are just props in the display of their own imagined superiority.

My latest piece on Time.com, The Breastfeeding Police Are Wrong About Formula, addresses new research that shows that early supplementation with formula actually improves rates of extended breastfeeding. Contrary to the dire predictions of lactivists, giving hungry babies formula until their mothers’ milk comes in does not sabotage breastfeeding.
It’s not surprising when you consider anthropological research that shows that early supplementation is common in a wide variety of cultures from the Indian subcontinent, to Southeast Asia to Africa. Mothers around the world, who fully intend to breastfeed for years, and do breastfeed for years, see nothing wrong with giving a baby supplements in the first few days after birth. So why have lactivists insisted that supplements sabotage breastfeeding and advocate letting babies scream for hours in hunger until a woman’s milk comes in?
It’s very simple; they value ideological purity over the wellbeing of babies.
Consider the Baby-Friendly Hospital Initiative, bizarrely named since it is not friendly to babies or to mothers. It is being implemented in hospitals around the country despite the fact that there is no evidence that it works and quite a bit of evidence that it does not. Indeed a paper published in the April 2013 issue of the journal Pediatrics found the opposite. According to the authors of Baby-Friendly Hospital Accreditation, In-Hospital Care Practices, and Breastfeeding:
…After adjustment for significant maternal, infant, clinical, and hospital variables, women who birthed in BFHI-accredited hospitals had significantly lower odds of breastfeeding at 1 month (adjusted odds ratio 0.72, 95% confidence interval 0.58–0.90) than those who birthed in non–BFHI-accredited hospitals. BFHI accreditation did not affect the odds of breastfeeding at 4 months or exclusive breastfeeding at 1 or 4 months…
When you consider the 10 steps of the Baby-Friendly Hospital Initiative, it’s hardly surprising that they don’t increase breastfeeding rates. Instead of addressing the problems that mothers identify — pain, difficulty, low milk supply, inconvenience — the 10 steps identify the problem that lactivists insist, without evidence, is responsible for low breastfeeding rates — cultural pressure.
Having misidentified the problem as a lack of ideological commitment, lactivists have misidentified the solution as greater enforcement of ideological purity.
Why is there such a massive disconnect between what works to improve breastfeeding rates and what lactivists recommend? Because lactivists aren’t really interested in the wellbeing of babies. They’re invested in boosting their own self-esteem by having their personal choices mirrored back to them … and punishing those who refuse to copy them by making them feel like bad mothers.
CDC statistics show that rates of combo-feeding (breastfeeding plus supplementation) exceeds rates of exclusive breastfeeding by 30 percentage points, demonstrating that large numbers of women are already successfully combining breastfeeding and supplementation. Anthropological studies show that women from many different cultures do the same. It’s time to re-orient our breastfeeding recommendations toward what actually works for babies and mothers, and away from the ideological purity demanded by lactivists.
It’s time for breastfeeding without guilt.